Healthcare Tim Worstall 27/01/2016 Healthcare Tim Worstall 27/01/2016 We can't help but think that numbers are important Read More Healthcare Tim Worstall 23/01/2016 Healthcare Tim Worstall 23/01/2016 Isn't this the point of the NHS in the first place? Read More Healthcare Tim Worstall 20/01/2016 Healthcare Tim Worstall 20/01/2016 Why we need to reform the NHS Read More Healthcare Tim Worstall 16/01/2016 Healthcare Tim Worstall 16/01/2016 A simple guide to us all being fatty lardbuckets Read More Healthcare Tim Worstall 14/01/2016 Healthcare Tim Worstall 14/01/2016 We're afraid that it's true, maternity leave does contribute to the gender pay gap Read More Healthcare Tim Worstall 13/01/2016 Healthcare Tim Worstall 13/01/2016 I'm afraid the doctors have this the wrong way around about the NHS Read More Healthcare Kate Andrews 12/01/2016 Healthcare Kate Andrews 12/01/2016 Five facts that undermine the junior doctors' strike Read More Healthcare Tim Worstall 10/01/2016 Healthcare Tim Worstall 10/01/2016 That tricky point about competition in the NHS Read More Healthcare Annabel Denham 07/01/2016 Healthcare Annabel Denham 07/01/2016 The Junior Doctors Row: Striking Won't Help Read More Healthcare Tim Ambler 07/01/2016 Healthcare Tim Ambler 07/01/2016 Can National Health Sense Be Dawning? Read More Healthcare Kate Andrews 11/12/2015 Healthcare Kate Andrews 11/12/2015 More evidence that the NHS is providing substandard care Read More Healthcare Tim Worstall 02/12/2015 Healthcare Tim Worstall 02/12/2015 Well, doesn't this just kill the Marmot Review Read More Newer Posts Older Posts Your subscription could not be saved. Please try again. Your subscription has been successful. Blogs by email Enter your email address to subscribe I agree to receive your newsletters and accept the data privacy statement. SUBSCRIBE
Healthcare Tim Worstall 27/01/2016 Healthcare Tim Worstall 27/01/2016 We can't help but think that numbers are important Read More
Healthcare Tim Worstall 23/01/2016 Healthcare Tim Worstall 23/01/2016 Isn't this the point of the NHS in the first place? Read More
Healthcare Tim Worstall 20/01/2016 Healthcare Tim Worstall 20/01/2016 Why we need to reform the NHS Read More
Healthcare Tim Worstall 16/01/2016 Healthcare Tim Worstall 16/01/2016 A simple guide to us all being fatty lardbuckets Read More
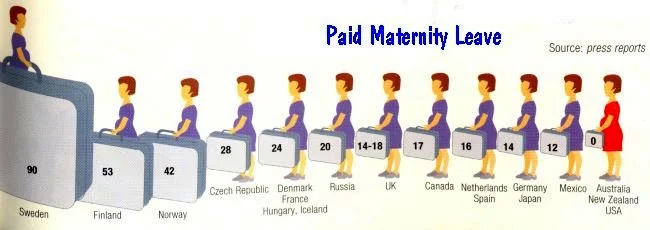
Healthcare Tim Worstall 14/01/2016 Healthcare Tim Worstall 14/01/2016 We're afraid that it's true, maternity leave does contribute to the gender pay gap Read More
Healthcare Tim Worstall 13/01/2016 Healthcare Tim Worstall 13/01/2016 I'm afraid the doctors have this the wrong way around about the NHS Read More
Healthcare Kate Andrews 12/01/2016 Healthcare Kate Andrews 12/01/2016 Five facts that undermine the junior doctors' strike Read More
Healthcare Tim Worstall 10/01/2016 Healthcare Tim Worstall 10/01/2016 That tricky point about competition in the NHS Read More
Healthcare Annabel Denham 07/01/2016 Healthcare Annabel Denham 07/01/2016 The Junior Doctors Row: Striking Won't Help Read More
Healthcare Tim Ambler 07/01/2016 Healthcare Tim Ambler 07/01/2016 Can National Health Sense Be Dawning? Read More
Healthcare Kate Andrews 11/12/2015 Healthcare Kate Andrews 11/12/2015 More evidence that the NHS is providing substandard care Read More
Healthcare Tim Worstall 02/12/2015 Healthcare Tim Worstall 02/12/2015 Well, doesn't this just kill the Marmot Review Read More